
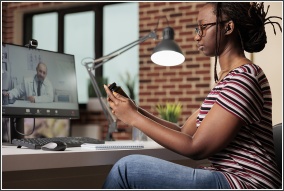
 There is an informative video by Sarah Wakeman on the physical and psychological perils of severe opioid withdrawal. Sarah is a Medical Director at Mass General Brigham. They are an integrated health care system that conduct medical research, teaching, and patient care.
There is an informative video by Sarah Wakeman on the physical and psychological perils of severe opioid withdrawal. Sarah is a Medical Director at Mass General Brigham. They are an integrated health care system that conduct medical research, teaching, and patient care.
In the video, Sarah explains how opioid withdrawal can become so severe with diarrhea and vomiting that individuals can die from extensive dehydration. As physicial dependency progresses, the brain becomes increasingly imbalanced and unable to function without the presence of opioids.
When opioid withdrawal commences (usually 8-12 hours after last use), it becomes increasingly unbearable as the body is flushed with stress hormones. The withdrawal discomfort builds in intensity over days, and can last up to a week or more. For many, this withdrawal process feels akin to a severe case of the flu, but then potentially reaches levels of sickness even far beyond that.
In the video, Sarah goes on to discuss the benefits of methadone and buprenorphine in reducing severe withdrawal symptoms and in helping patients to ultimately not die from overdose. She also illuminates on how rational decision-making is so extremely difficult when struggling against the intense pain of opioid withdrawal.
Please check this video out, and share it with anyone you believe can benefit from its message.
 Follow
Follow

 There’s a new spin being proposed on the dispensing of methadone to Opioid Use Disorder (OUD) patients. A federally-funded
There’s a new spin being proposed on the dispensing of methadone to Opioid Use Disorder (OUD) patients. A federally-funded  The U.S. Dept. of Health and Human Services has awarded $1.5 billion in an effort to support States in their fight against opioid addiction.
The U.S. Dept. of Health and Human Services has awarded $1.5 billion in an effort to support States in their fight against opioid addiction.  Providence, Rhode Island is the first location in the United States to offer a mobile methadone service. This
Providence, Rhode Island is the first location in the United States to offer a mobile methadone service. This 
